
From the 1Centre of Expertise in Rehabilitation and Audiology, Adelante Rehabilitation Centre, 2Department of Amputation, Traumatology and Orthopaedics, Adelante Rehabilitation Centre, Hoensbroek, 3Department of Rehabilitation Medicine, Zuyderland, Heerlen, 4Trauma Centre Limburg, Maastricht University Medical Centre, 5Department of Rehabilitation Medicine, Research School CAPHRI, Maastricht University, Maastricht and 6Libra Rehabilitation and Audiology, Eindhoven/Weert, The Netherlands
Objective: To assess the availability of explicitly reported protocols describing post-surgery rehabilitation of (peri-)articular fractures of the proximal humerus, acetabulum and/or tibial plateau, and to critically review any scientific evidence on the effectiveness of these protocols.
Data sources: MEDLINE (PubMed), Cochrane databases, CINAHL, PEDro and Embase (Ovid) were searched to November 2018. Furthermore, stakeholder internet sites, clinical guidelines and standard textbooks were searched.
Study selection: Screening was performed independently by 2 researchers based on a priori defined eligibility criteria.
Data synthesis: Five papers addressed post-surgical rehabilitation of proximal humerus fractures, one paper addressed acetabulum fractures. No eligible information was found on stakeholder sites or in standard textbooks. Overall, the main focus of the protocols identified was on the International Classification of Functioning, Disability and Health (ICF) “Body Functions and Structures” level. In general, little information about therapy dosage was reported. None of the protocols provided scientific evidence on which the content of described rehabilitation programmes was based.
Conclusion: This review reveals a paucity of explicitly formulated protocols focussing on post-surgical rehabilitation of common (peri-)articular fractures targeting patient-centred care at all ICF levels. There
is a need for more scientific evidence on which to base protocols regarding common (peri-)articular fracture rehabilitation.
Key words: rehabilitation; aftercare; (peri-)articular fractures; therapy protocol; systematic review; tibial plateau; proximal humerus; acetabulum.
Accepted Aug 21, 2019; Epub ahead of print Sep 5, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Henk A. M. Seelen, 1Centre of Expertise in Rehabilitation and Audiology, Adelante Rehabilitation Centre, Hoensbroek, the Netherlands. E-mail: h.seelen@adelante-zorggroep.nl
The aim of this study was to review the scientific literature on the availability of explicitly reported protocols or guidelines for therapists describing rehabilitation treat-ment of patients with one or more complex fractures of the upper arm, pelvis or knee joint that needed to be operated on. Online databases, stakeholder internet sites, clinical guidelines and textbooks were searched. The papers found were critically reviewed. Five papers describing the rehabilitation of patients with an upper arm fracture and one paper on rehabilitation treatment after a pelvis fracture were identified, mainly describing muscle strength, joint mobility or endurance issues. Little information about therapy dosage was reported. No scientific evidence was provided on which to base the rehabilitation programmes. This review reveals a lack of explicitly formulated rehabilitation protocols focusing on improving patients’ activities of daily living and of patients’ participation in social life. More scientific evidence is needed on such protocols.
Bone fractures sometimes require reduction and internal fixation. These fractures are relatively simple to treat and rarely result in functional limitations. However, depending on the location, nature, complications and healing process, some fractures are more complex to reduce and fixate. In general, peri- and intra-articular fractures are more demanding. In addition, the adjacency of the fracture fixation to the joints makes after-treatment more challenging. The choice of rehabilitation protocol depends on the reduction and fixation strategy used. Clinical practice has shown that rehabilitation greatly influences the recovery of the patient (1–4).
In current clinical practice, rehabilitation is provided according to the International Classification of Functioning, Disability and Health (ICF) (5). This classification specifies 3 levels of functioning, i.e. the “Body Functions and Structures” level, the “Activity” level and the “Participation” level. The ultimate goal of rehabilitation therapy is to improve the functioning of the patient at the Activity and Participation levels.
Whereas a myriad of information is available on the (surgical) reduction and fixation procedures and protocols of (peri-)articular fractures, as well as on the processes involved in bone healing (e.g. www.aofoundation.org), the ensuing rehabilitation aftercare, or rehabilitation, seems less systematically documented and is often based on empirical, implicit knowledge of the individual (para-)medical specialist or therapist. Although aftercare is mentioned as being very important in the treatment of patients with (peri-)articular fractures, description of its exact content is rare. To identify which physiotherapy/occupational therapy protocols for the post-surgery treatment of (peri-)articular fractures have been published and to assess their quality, a systematic literature search was performed. To enhance the clarity of this search, 3 types of (peri-)articular fractures were considered; proximal humerus fractures, tibial plateau fractures, and acetabulum fractures.
The aims of the current study were: (i) to assess the availability of explicitly reported physiotherapy/occupational therapy protocols or formal guidelines describing rehabilitation following surgery of (peri-)articular fractures of the proximal humerus, the acetabulum and/or tibial plateau; and (ii) to critically review the scientific evidence on the effectiveness of (parts of) these protocols.
Data sources
A computerized search was conducted of all English, French, German and Dutch scientific papers in MEDLINE (PubMed), Cochrane databases, CINAHL, PEDro and Embase (Ovid). Studies were collected up to November 2018. The following Medical Subject Headings (MeSH) were used: (“Acetabulum” OR (“Humerus” AND “Proximal”) OR (“Tibia” AND “Plateau”)) AND “Fracture” AND (“Rehabilitation” OR “Physical Therapy”) NOT “Infant” NOT “Pediatric” NOT “Animal” NOT “Cadaver” NOT “Equipment Design” NOT “Case Report” NOT “Legislation”.
Furthermore, a search for possible guidelines as to rehabilitation therapy content regarding aftercare following surgery for (peri-)articular fractures was performed on a number of stakeholder sites on the internet (in the domain of surgery and traumatology: www.aofoundation.org; in the domain of medical audit: www.diliguide.nl/richtlijnen/professionals; in the domain of rehabilitation sciences: Dutch Paramedical institute (NPI): www.paramedisch.org/doconline/portal.html; and clinical practical guideline domain: http://guidance.nice.org.uk, www.sign.ac.uk, http://guidelines.gov, http://ww2.rch.org.au, https://www.mja.com.au, http://www.evidence.nhs.uk). Finally, standard textbooks covering issues related to the treatment of (peri-)articular fractures, recommended by the Taskforce Trauma Rehabilitation (Dutch: WTR) of the Dutch Society of Rehabilitation Medicine (Dutch: VRA), were checked.
Study selection
All papers identified by the search strategy were checked for duplicates. A language check was also performed.
Two independent observers conducted the paper selection in 2 steps:
1) Based on the papers’ title and abstract, first a global exclusion cycle was performed, identifying papers that definitively did NOT contain ANY indication AT ALL concerning a rehabilitation protocol or aftercare protocol, or an indication related to fractures of the proximal humerus, acetabulum or tibial plateau. Also, animal studies, model studies or single-case descriptions were excluded. In case of any doubt, the paper was not excluded in this phase of the selection procedure.
2) Next, based on the full text of the papers, documents were evaluated with regard to 4 additional (sequential) criteria:
a) Is the term “aftercare”’ (or any equivalent term) mentioned and specified in any way? (Y/N);
b) Are any treatment aims and treatment elements (e.g. mobilization) mentioned? (Y/N);
c) Is any treatment content described in terms of nature and/or time and/or intensity? (Y/N);
d) Are any decision rules and/or decision moments regarding the provision of therapy described? (Y/N);
Papers were considered eligible if the answer to all 4 questions mentioned above was “yes”. In case of inter-observer disagreement, the paper was discussed by the 2 observers. Consensus was reached in all cases.
Data extraction
The results of the literature search are reported per fracture location. First, the rehabilitation programmes are described in general. Then, the content of the post-surgical rehabilitation programmes is systematically described in the text and classified in a table according to: (i) ICF-level targeted (Function, Activity, Participation) (5); (ii) time course (treatment phases, i.e. time-delimited epochs within the rehabilitation process in which the therapy is focused on one or more specific treatment goals); (iii) goal(s) strived for; (iv) therapy dosage (i.e. frequency, duration and intensity of therapy). Furthermore, the programmes were assessed as to the availability of decision rules determining the timing of the initiation of new therapy elements, training specificity (i.e. whether aftercare focused on the whole body (in general) or on a specific body region), and whether protocols accommodate for adjustments to individual patients’ needs. In addition, for evaluating the scientific evidence as to the effectiveness of (parts of) the protocols identified, the Van Tulder’s Quality assessment system was used (6). For descriptive analysis, the Patients, Intervention, Comparison and Outcome & Results (PICO) principle (7) was followed.
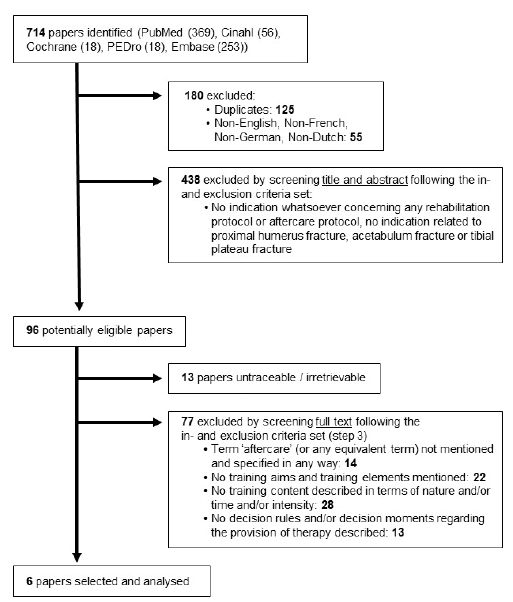
The initial literature search resulted in 664 papers. Removal of duplicates resulted in 549 papers and, after a language check, a further 54 papers were removed, leaving 495 documents for assessment in step one. Based on a global evaluation of the articles’ titles and abstracts, 284 articles were excluded. Of the remaining 211 papers, 80 remained after the assessment of step 2. Next, 13 papers were excluded, because no full-text could be retrieved. After the evaluation in step 3, another 61 articles were excluded, resulting in 6 eligible papers. A flowchart of the selection process is shown in Fig. 1. No eligible information was found on stakeholder sites or in standard textbooks.
Fig. 1. Flowchart paper selection.
Content description
Of the 6 eligible papers, 5 addressed physiotherapeutic/occupational therapeutic rehabilitation after surgical treatment of proximal humerus fractures (1, 2, 8–10) and one addressed post-surgical physiotherapeutic/
occupational therapeutic rehabilitation of acetabulum fractures (4). No paper describing the rehabilitation of tibial plateau fractures met the selection criteria. Background information about the protocols selected is shown in Table I.
Table I. Background information protocols selected
Proximal humerus fractures
In the selected papers, a rehabilitation specialist or physical therapist supervised the post-surgical rehabilitation of proximal humerus fractures. According to Compito et al. (8) the therapy was especially aimed at: (i) recovery, and then (ii) preservation of motion of the glenohumeral complex. All authors described a general physiotherapy/occupational therapy training programme, making no distinction between either the complexity of the fracture, (surgical) reduction or fixation type. The research group of Handoll et al. (10) prescribed a physiotherapy/occupational therapy protocol that was used for both post-surgical rehabilitation and conservative treatment. The extent to which the papers selected reported the post-surgical therapy programme differs considerably, varying from a brief description of the exercises (1, 9, 10) to a more specified protocol including exceptions where the protocol explicitly should not be followed and the underlying thoughts for this protocol deviation (2, 8). However, all authors seem to agree on the general therapy content and progression of the post-fracture rehabilitation process, though the explicit arrangement into phases is dissimilar. Based on this observation, the findings of all 5 papers were combined, as presented below.
ICF – Body Functions and Structures level. According to Moeckel et al. (9), the first phase of the selected rehabilitation therapy programmes was aimed at gaining full passive range of motion, i.e. improving joint mobility, without compromising the stability of the fixation. In the protocol of Handoll et al. (10), the first phase was aimed at prevention of comorbidities through, for instance, elbow, wrist and hand exercises, and teaching sling application and axillary hygiene. All other protocols strived for optimizing joint mobility through pendulum exercises, passive forward elevation and passive external rotation, starting the first day post-operatively. In the protocol of Handoll et al. (10) these exercises were initiated in the second phase. The surgeon defined during surgery (2, 9) or on the first post-operative day (8), the range of motion constraints during the exercises. In contrast to the other authors, Compito et al. (8) stated that the patients should use a sling for 6 weeks, except during therapy activities (8). Patients receiving rehabilitation according to the protocol of Handoll et al. (10) should wear a sling for approximately 3 weeks, including during exercises. When the patient feels safe, the sling can be removed during exercises. According to Burton & Watters (1) patients should warm-up by using a warm pack on the shoulder. Patients receiving rehabilitation therapy in accordance with the protocols of Cuomo et al. (2) and Burton & Watters (1) had to repeat the exercises 4 times daily. Handoll et al. (10) advised therapists to instruct patients to perform 5 repetitions, 3 times per day, of all exercises in all phases. Compito et al. (8) and Moeckel et al. (9) provided no information about the training frequency and duration within this phase.
The therapy in the second phase showed a larger variation across post-surgical therapy programmes. Although in all papers the second phase was reported to start at around the same time, i.e. approximately 6 weeks post-trauma, different clinical reasoning substantiating the start of phase 2 was used. The main focus in this phase was the improvement in joint mobility and strength. Overall, the second phase of the physiotherapeutic/occupational therapeutic treatment programme consisted of active assisted exercises and strengthening or resistive exercises, though the exercises were executed differently. In addition to these exercises, stretching exercises were prescribed by Burton & Watters (1) and Handoll et al. (10). Handoll et al. (10) added isometric rotation exercises and closed chain exercises. Due to insufficient information about the therapy dosage, it was not possible to explore whether therapy could improve endurance.
The third and last phase, starting approximately 3 months post-trauma, was mostly aimed at improving the strength through resistive strengthening exercises. Similar to the second phase, too little information was provided to explore whether therapy aimed at improv-ing endurance. Except for the programme described by Moeckel et al. (9), mobility was improved by using stretching exercises. Exercises were not specified, e.g. regarding movement plane. In contrast to the other protocols, Burton & Watters (1) and Handoll et al. (10) started out putting more emphasis on the needs of the individual patient, by stating that aftercare should continue “until functional gain reaches a plateau or pre-injury levels” (1) or to continue strengthening exercises “appropriate to the patient’s premorbid activity level” (10). In current rehabilitation therapy, this approach has been further developed into what is called “’patient-centred” rehabilitation, in which individual goal setting and patient-specific training regimes are advocated. The duration of the full rehabilitation programme varied from approximately 1 year (8, 9), to 1 year and 3 months (2). Handoll et al. (10) prescribed to discharge patients when independent shoulder function is achieved or if the therapist and patient do not observe any improvement over several sessions.
Assessment rules based on patient characteristics or on the progression of the fracture recovery seem to be missing in most phases of the papers selected, though Handoll et al. (10) state that the progression of the rehabilitation process is dependent on certain factors, e.g. stage of healing, and general health and activity level. As a result, these papers only provided a general roadmap instead of a protocol targeting aftercare at an individual level. Furthermore, no methods to objectively monitor the rehabilitation progress were mentioned. In addition, the papers only described the physiotherapeutic/occupational therapeutic treatment for fracture rehabilitation, disregarding possible other physical or mental consequences of the fracture.
Moreover, none of the papers reported scientific evidence on which the described physiotherapy/occupational therapy protocols were based. Furthermore, only Handoll et al.’s research group (10) examined and confirmed the effectiveness of their therapy protocol (for methodological quality assessment, see below).
ICF – Activity level. In the second and third phase, patients receiving therapy according to the protocol of Handoll et al. (10) should progress functional activities consistent with their abilities. However, no further description of the content of these activities was given. In the other papers selected, no rehabilitation therapy that focuses on the ICF activity level was provided.
ICF – Participation level. No explicit interventions that focus on the ICF participation level were described in either of the post-surgical rehabilitation programmes selected.
Acetabulum fractures. The paper by Maurer et al. (4) addressed the physiotherapeutic/occupational therapeutic rehabilitation of acetabulum fractures after surgical as well as conservative treatment, although in the present paper we only outline the post-surgical rehabilitation programme. Maurer et al. (4) described the therapy in more detail compared with the papers addressing the rehabilitation of proximal humerus fractures. Furthermore, the rehabilitation programme focussed not only on recovery of the affected region, but also on maintaining the mobility and strength of the contralateral side and on possible risks of the patients being bedridden, e.g. prevention of pneumonia and thrombosis. The goal of the post-surgical therapy was restoring painless functioning of the affected joint towards pre-injury level with concomitant levels of full weight-bearing associated with stance and gait.
ICF – Body Functions and Structures level. The protocol is subdivided into, what are termed 4 successive “mobilization phases”, implying that the focus of the therapy was mostly on the ICF Body Functions and Structures level. In the first phase, only therapy related to mobility, i.e. traction and stretching, and muscle strength was provided. During this first phase, patients were immobilized. Patients lay in bed in the supine position with traction in the longitudinal direction of the affected bone. Furthermore, treatment aimed to preserve the mobility, muscle strength and coordination of both lower limbs using the propriocep-tive neuromuscular facilitation (PNF) technique (12). Therapy dosage was not mentioned.
In the second phase, the therapy was expanded, but still only targeting the mobility. It was stated that PNF treatment was continued, although the therapy content was not specified. The appliances for the positioning in bed, such as foamed splints, were removed in order to enlarge the mobility of the hip joint. The goal was to: (i) mobilize the affected hip by using small movements with little or no weight-bearing; and (ii) improve muscle strength and coordination, according to the functional kinetics of Klein-Vogelbach (13). Furthermore, movements of single gait phases were practiced passively in bed. The frequency and duration of the therapy and exercises were not mentioned. Besides the hip joint of the affected limb the ipsilateral knee joint was trained in this second phase.
The third phase of the programme started in the third week post-trauma. The traction in the longitudinal direction of the affected bone was removed. Mobilization of the affected limb was continued in this phase. Previously trained PNF-related movement transitions and patterns were now used during the training of sitting, gait and stance. Patients could participate in group hydrotherapy to train non-weight-bearing and group remedial therapy focussing on stabilization and the mobility of the knee joint. The content of both group sessions was not specified. Due to a lack of information about the therapy dosage, it was not possible to assess whether the therapy in this phase improved endurance.
In the fourth and last phase, patients received treatment in an outpatients’ department. Patients could be discharged from the hospital when the muscles could secure the mobility of the affected hip joint and the gait pattern corresponded with the physiological gait pattern. In this last phase, reaching full loading of the affected joint at approximately 10 weeks post-trauma was aimed for by gradually increasing the loading of the injured limb. No information was provided about the assessment of weight-bearing. Exercises and other therapy components performed in this phase were not specified. Furthermore, therapy frequency and duration were not specified.
Similar to the protocols on proximal humerus fractures, assessment rules based on patient characteristics or on the progression of the fracture recovery were missing in most phases of this protocol. In addition, no methods to objectively monitor the rehabilitation progress were mentioned. Patient-specific care cannot be provided on the basis of this protocol. Although care was provided for physical consequences of the fracture, possible psychological consequences were disregarded.
The authors did not provide scientific evidence on which to base the rehabilitation programme described, and did not scientifically examine the effectiveness of their programme.
ICF – Activity level. In addition to the previously described therapy in the third phase, the post-surgical rehabilitation programme also provided therapy focussing on the ICF activity level. In this phase, patients were allowed to walk with the aid of elbow crutches loading the affected limb to a maximum of 20 kg. How this weight was controlled was not described. Therapy focusing on the ICF activity level was not provided in any of the other phases.
ICF – Participation level. No therapy aims on the ICF level of participation were described. In Table II, the content of the physiotherapy/occupational therapy programmes selected, is summarized.
Descriptive analysis and methodological assessment of the effectiveness of the studies
In the present paper, descriptive analysis and metho-dological assessment of studies examining the effectiveness of the protocols of the eligible papers was strived for. However, only the papers of Handoll et al. (10) and Moeckel et al. (9) reported on effectiveness obtained from clinical trials, whereas the rehabilitation protocols of Burton & Watters (1), Compito et al. (8), Cuomo & Zuckerman (2), and Maurer et al. (4) were not studied for their effectiveness. Furthermore, the aim of the clinical trial reported on by Moeckel et al. (9) was not within the scope of the present paper, i.e. the focus was not on evaluation of the rehabilitation protocol. Consequently, we only performed the methodological assessment and descriptive analysis for the effectiveness study described by Handoll et al. (10). This methodological assessment resulted in a total Van Tulder score of 12 out of 19. The subscores for internal validity, descriptives and statistics were 6 out of 11, 4 out of 6, and 2 out of 2, respectively (for scores see Appendix 1).
The results of the descriptive analysis of the effectiveness study performed by Handoll et al. (10) are presented in Table III. Handoll et al. (10) equally allocated 250 patients with proximal humerus fractures to either an intervention group or a control group. In 193 of the patients included in the study, tuberosity involvement was identified. In the intervention group surgical treatment of the fracture was provided and rehabilitation according to the protocol described under “Content description” in the present paper. Patients allocated to the control group received non-surgical treatment of the fracture with similar rehabilitation treatment. No statistically or clinically significant differences were found between the groups.
Table II. Overview of the time phases/load-bearing epochs and the treatment activities performed
Table III. Descriptive analysis of effectiveness study of Handoll et al. (10)
The aims of this review were: (i) to assess the availability of explicitly reported physiotherapy/occupational therapy protocols or formal guidelines describing rehabilitation following surgery of (peri-)articular fractures of the proximal humerus, the acetabulum and/or tibial plateau; and (ii) to critically review any scientific evidence on the effectiveness of (parts of) these protocols.
In general, many authors state that rehabilitation is as important as proper fracture reduction and fixation, although only a few authors describe their rehabilitation protocol extensively. Regarding the post-surgical rehabilitation of fractures of the proximal humerus, acetabulum and tibial plateau, 6 eligible papers (1, 2, 4, 8–10) were found, of which 5 discussed the rehabilitation of proximal humerus fractures (1, 2, 8–10) and 1 the rehabilitation of acetabulum fractures (4). No paper addressed protocols for the post-surgical rehabilitation of tibial plateau fractures. It should be noted that 4 out of the 6 papers identified were published in the 1990s. However, interest in the rehabilitation of, especially, proximal humerus fractures seems to be increasing (1, 10, 14). It is necessary to investigate protocols on their effectiveness and report on new research and trends to be able to improve rehabilitation of (peri-)articular fractures. However, of the protocols selected, only the protocol of Handoll et al. (10) was studied for its effectiveness.
The extent to which the papers describe the therapy varies widely. In general, little information is given about therapy dosage. As opposed to the rehabilitation programmes for proximal humerus fractures, the post-surgical rehabilitation programme for acetabulum fractures (4), identified as being relevant for this study, targeted the whole body instead, like prevention of pneumonia and thrombosis. In general, the post-surgical rehabilitation protocols identified in our review focus on the ICF body function level, possibly since most papers have been published many years ago. Remarkably, in none of the protocols was scientific evidence provided on which the described rehabilitation programmes were based.
In contrast to the literature on the rehabilitation of some fractures after surgical treatment, more information is available about the rehabilitation of fractures after conservative treatment, like the papers of Limb (15) and Wiedemann & Schweiberer (16). As the timing and approach of the rehabilitation of these fracture types differs, distinct protocols for each type of rehabilitation aftercare, be it after surgical or non-surgical intervention, are needed (14).
Methodological considerations
In the present paper a descriptive analysis and metho-dological assessment could only be performed of the paper of Handoll et al. (10). Performing either or both of these assessments of the other papers selected was not possible or relevant because: (i) psychometrically well-defined tools to assess clinical treatment protocols regarding the aftercare treatment of (peri-)articular fractures seem to be lacking in literature; (ii) the effectiveness of the protocols in the papers selected was not established, disallowing the use of tools to assess clinical trials or intervention studies like the Van Tulder’s Quality assessment system or the PICO principle; and (iii) the aim of the paper selected (i.e. Moeckel et al. (9)) was not within the scope of the present paper.
Conclusion
In conclusion, our review reveals a paucity of explicitly formulated rehabilitation protocols focussing on the post-surgery treatment of some (peri-)articular fractures. The available protocols contain only a brief description and lack therapy-related details, e.g. therapy dosage and criteria to evaluate adjustment of dosage or type of training. There was a notable lack of rehabilitation protocols targeting patient-centred care at all ICF levels, based on scientific evidence on the effectiveness of (parts of) these protocols, that systemically describe the whole aftercare process. In future, protocols including detailed information on these components need to be realized in order to facilitate testing their (cost-)effectiveness and systematic implementation in other centres.
Appendix 1. Van Tulder’s quality assessment system. From: Handoll et al. (10).


 Click to show fullsize
Click to show fullsize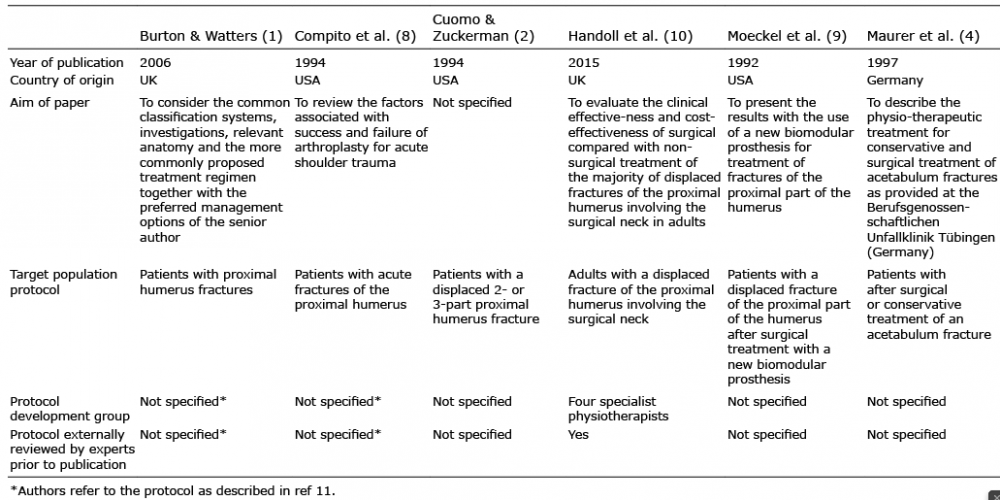 Click to show fullsize
Click to show fullsize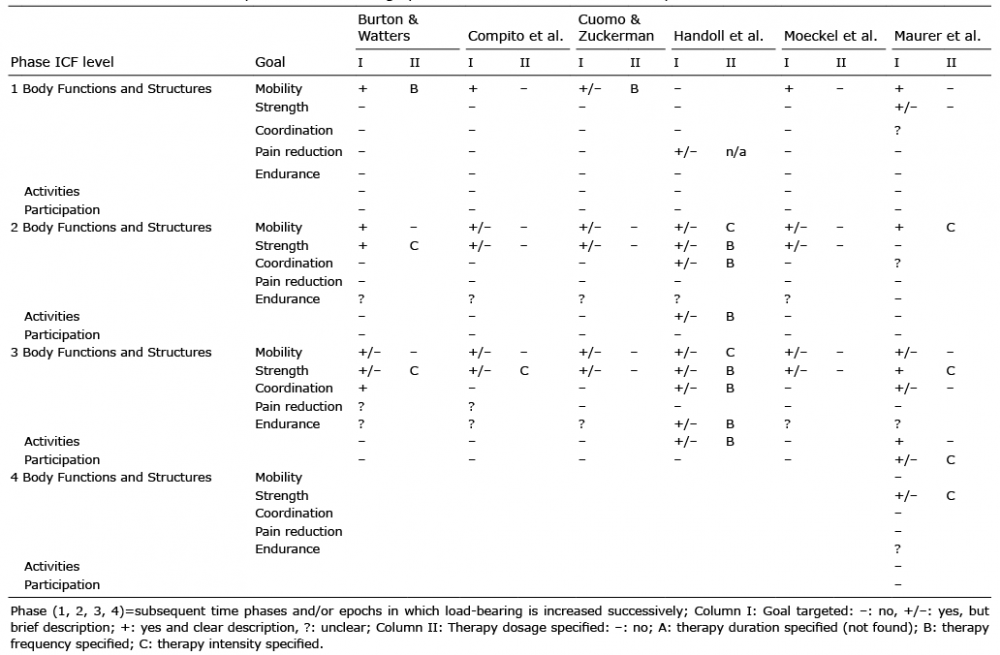 Click to show fullsize
Click to show fullsize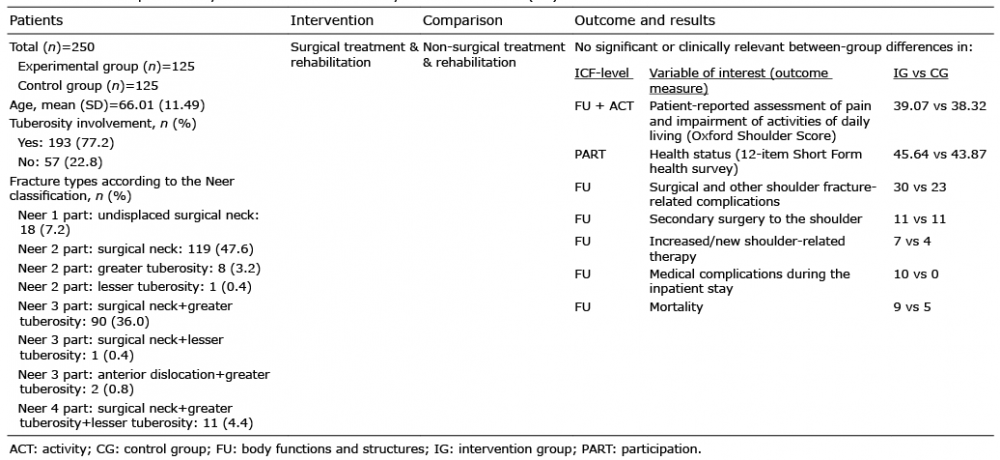 Click to show fullsize
Click to show fullsize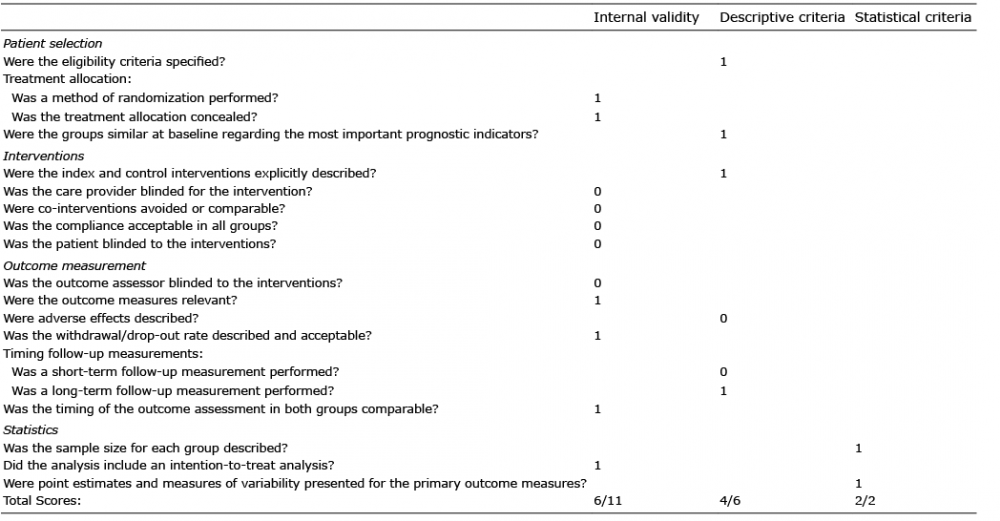 Click to show fullsize
Click to show fullsize